Medicare pricing changes could cost comp
Reprints
The Centers for Medicare & Medicaid Services recently updated its reimbursement rates for medical services, and experts are monitoring how the changes may affect workers compensation medical fee schedules and insurance rates.
The extent of the effect on workers comp will vary by jurisdiction because some states base comp medical fee schedules on Medicare while others do not. But any change to medical costs is seen as an area to watch in comp, as the industry pays attention to medical inflation as a potential cost-driver. The rate changes were less than 2% (see related story below).
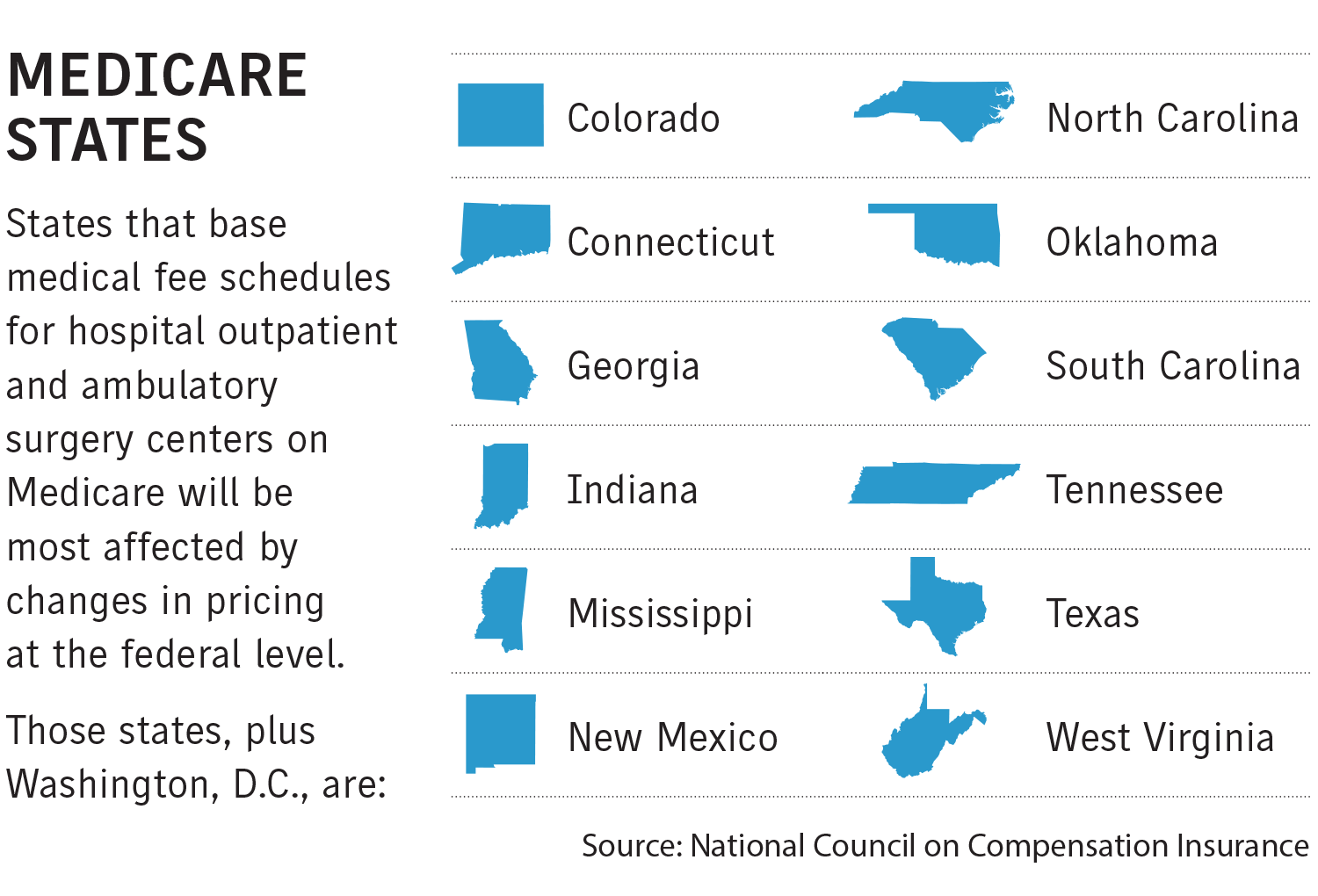
States that base their fee schedules on Medicare automatically incorporate the changes into their updated schedules, while other states may use them as a benchmark, the Boca Raton, Florida-based National Council on Compensation Insurance said in a report in April addressing the annual CMS update.
“Some states may completely ignore what CMS is doing in setting their own rates,” said NCCI actuary Jon Sinclair, one of the report’s coauthors. “It’s sort of hyper-specific to each state how their fee schedules work and what they consider each year when updating them.”
Any immediate effect on insurance rates is also unknown, and rates may increase or decrease, said Steve Bennett, Washington-based assistant vice president for workers compensation programs and counsel for the American Property Casualty Insurance Association. “That will be up to the statistical rating organizations to see how those play out.”
A spokesman for the New York State Workers’ Compensation Board said the CMS updates will not directly affect rate settings in that state’s comp system.
“CMS data is only one of several factors that the board considers when it periodically updates its various fee schedules,” he said.
Alex Swedlow, president of the California Workers’ Compensation Research Institute, said updating fee schedules can have a direct effect on the cost of medical care in comp, but that other factors are taken into consideration.
“There are so many additional inputs to rates in an open rating environment like California that it would be hard to put a percentage on how much a (CMS) rate change influences the rates,” Mr. Swedlow said.
While California is a “very expensive state as measured by loss adjustment expenses and frequency, our fee schedules for medical care are largely established at 120% of Medicare. That means we’re reimbursing at 20 points better than the largest payer in the state,” Mr. Swedlow said.
CLICK IMAGE TO ENLARGE
Charles Cordova, an economist with the New Mexico Workers’ Compensation Administration, said in an email that he expects the CMS changes to result in a small overall increase in medical costs in the state’s comp system, and any rate change will be minor compared with normal market fluctuations.
While CMS increased reimbursement rates for facilities, as well as for durable medical equipment and supplies, it decreased payment rates for physician services this year, and physician costs make up about 40% of nationwide medical expenditures in comp, according to the NCCI.
Many states base their physician fee schedules on CMS reimbursement rates.
Providers are unlikely to refuse comp patients if changes are pushed through, experts say.
“We wouldn’t expect any shifts in provider participation, as we’re always striving to maintain rates that are fair for providers and payers,” stated the spokesman for the New York State Workers’ Compensation Board.
Mr. Swedlow, of the CWCRI, said California has a provider shortage. In 2030, the state is projected to be short 34,000 doctors and 45,000 nurses.
“There’s very little workers compensation can do about that,” Mr. Swedlow said. “It’s not as if we can open up our own medical schools and hospitals to train future physicians and nurses. That’s a much more troubling issue in terms of dealing with the access to care problem.”
Ramona Tanabe, president and CEO of the Workers Compensation Research Institute, said if a state did look to decrease physician reimbursement rates in medical fee schedules, it would likely consider the effect it might have on comp patients.
“I don’t think any policymakers want to have the effect of impeding access to care for injured workers,” she said.
Medical inflation, high court ruling influence level of increases
Recent changes to medical service reimbursement rates by the Centers for Medicare & Medicaid Services may have the strongest effect on pricing for services at medical facilities, but much depends on the type of care a patient receives, according to experts.
Under the CMS updates, hospital inpatient facilities this year will receive a reimbursement rate increase of 1.4% while the rate for ambulatory surgery centers will go up by 1.9% from 2022.
Jon Sinclair, an actuary with Boca Raton, Florida-based National Council on Compensation Insurance, said CMS updates its base rates to account for changes in the prices of goods and services used by facilities in treating Medicare patients, which could affect comp.
Hospital outpatient and ambulatory surgery centers account for two-thirds of nationwide facility costs in workers comp; the remaining third comes from hospital inpatient facilities.
One reason for the 2023 facility base rate percentage increase is fallout from the U.S. Supreme Court decision in American Hospital Association v. Becerra, which concerned drug reimbursements for hospitals participating in a program that enables the purchasing of medications from drug manufacturers at discounted rates.
The high court ruled the Department of Health and Human Services improperly paid lower reimbursement rates to some hospitals that obtained the lower cost drugs because federal law doesn’t allow HHS to unilaterally make Medicare reimbursement cuts.
Kara Newbury, director of government affairs and regulatory counsel for the Alexandria, Virginia-based Ambulatory Surgery Center Association, wrote in an email that the only reason ambulatory surgical centers received a higher reimbursement rate than hospital outpatient facilities this year was the “anomaly” caused by the Becerra decision.
Ms. Newbury said ambulatory surgery centers are small businesses that receive no federal subsidies for providing care to comp patients and others, and thus need to remain profitable to stay open.
“Therefore, they cannot afford to perform large numbers of procedures for which the reimbursement does not cover the costs they incur to provide them,” Ms. Newbury wrote.
Ms. Newbury said hospital outpatient facilities have historically received much higher reimbursement rate increases than surgical centers, and that “future disparities remain uncertain until other rules are finalized.”
To assess the effect of Medicare payment rates and policies on comp, types of procedures would also need to be considered, she said.
Charles Cordova, an economist with the New Mexico Workers’ Compensation Administration, said ambulatory surgery center guidelines in his state are based on CMS rates, and that surgery center costs represent about 5% of total medical costs in the state, at an estimated $7.2 million.
He said this year’s CMS increase for surgery centers would likely only result in a total medical payment increase of about 0.2% in New Mexico.
