Comp sector explores physical medicine options
Reprints
As the workers compensation industry takes strides to limit opioid prescriptions and avoid invasive surgeries, hands-on physical medicine is getting more attention than ever.
Physical medicine — an umbrella term for physical therapy and other services that aim to rehabilitate injured workers — is increasingly seen as an early investment in patient care, with outcomes that can reduce recovery time off following an injury, experts say.
Although, in some instances extensive physical therapy can lead to higher costs, an analysis shows.
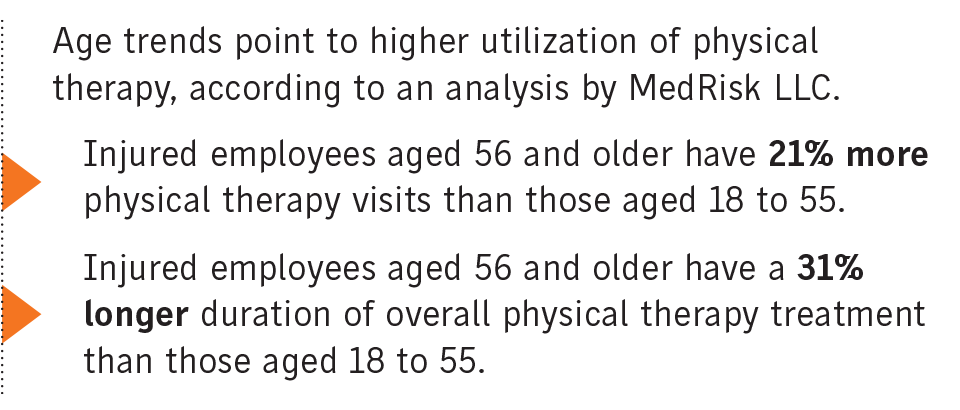
“We’re seeing opioid use going down, we’re seeing surgical rates going down, and we’re seeing therapy utilization going up,” said Brian Peers, King of Prussia, Pennsylvania-based vice president of clinical services and provider management for MedRisk LLC, which manages physical medicine services for injured workers.
MedRisk’s recent industry trends report describes physical medicine as “conservative care” that can cost more up front but pay dividends through lower overall treatment and workers comp.
In 2022, MedRisk continued to see a lower rate of surgery on claims involving physical therapy, a downward trend it began documenting in 2015 when just under 25% of claims involving physical therapy included a surgery component. In 2021 and 2022 that figure hovered at 16%.
Early manual therapy — a type of physical therapy — for injured workers with lower back pain was associated with lower utilization of medical services, lower medical and indemnity payments, and shorter disability, according to a September 2022 study by the Workers’ Compensation Research Institute.
Using data from 18 states representing a majority of U.S. comp spending, the Cambridge, Massachusetts-based institute found an average medical cost of $4,192 for lower back pain claims with early manual therapy, 27% lower than that for similar claims with late manual therapy.
Researchers also found that workers receiving manual therapy within two weeks of traditional physical therapy needed fewer MRIs, 30.3% versus 43.4%; received fewer opioid prescriptions, 18.6% versus 23.3%; and had fewer pain-management injections, 12.6% versus 16.5%.
And the average indemnity payment per claim was 28% lower when manual therapy was initiated early and the average temporary disability duration per claim was 22% shorter.
The move to more physical medicine was a natural progression in workers compensation, experts say.
“In health care, the push to minimize the footprint of opioids created a void, and the question became what would fill it,” wrote Michael Hough, assistant vice president of managed care for Sedgwick Claims Management Services Inc., in an email.
“Physical therapy has been a constant staple within the health care landscape, but the movement away from passive therapies — like opioid utilization — has given physical therapy an opportunity to better entrench itself.”
Effective physical therapy involves early intervention, adequate treatment time and attention to detail, experts said. But there are pitfalls and concerns, too.
A separate analysis of physical medicine services released by WCRI in February found claims with “extended” physical medicine use had higher overall medical costs, higher indemnity payments and a longer duration of temporary disability. A lack of coordination between providers was the likely cause of the costly extended care, the report said.
Severity indicators also predict extended physical medicine use, according to WCRI. For example, claims with nerve involvement were 2.4 times more likely to have extended physical medicine use relative to similar cases without neuropathic conditions. Workers with at least one comorbidity were 1.8 times more likely to have extended physical medicine visits. There’s also an element related to mental wellness (see related story).
Dr. Scott Cherry, chief medical officer for The Woodlands, Texas-based Axiom Medical Consulting Inc., said evidence-based care is essential when it comes to physical therapy. More isn’t always better, and one size fits all doesn’t always work, he said.
“It’s important to have a good sense of getting accurate information about each injury on a case-by-case basis, and then also getting a good assessment of severity. From there, you can kind of see what’s the most evidence-based approach to each type of injury,” he said. “There can be overuse of physical therapy when it’s not indicated, or if it’s not effective.”
Continuing physical therapy if it isn’t helping can hinder recovery, said Michelle Despres, Jacksonville, Florida-based vice president of physical therapy at One Call Care Management Inc.
“If somebody’s low back is hurting, often it’s chronic. … They’ve probably tried many things, and many things haven’t resolved their problem,” she said. “They’re coming into physical therapy, and they’re not getting better. Then it’s just one more on the list of things that didn’t work. We’re setting a person up to sort of affirm in their mind that they’re never going to be better.”
Patient buy-in and communication are also essential, Ms. Despres said.
If a patient isn’t improving, it’s important to determine the reason, she said.
