Updating medical fee schedules takes balance
Reprints
Medical inflation is a top concern in workers compensation this year and adjusting medical fee schedules may be one way to address rising costs, although the appetite for change is limited, comp experts say.
While some states have introduced legislation to overhaul their schedules, variations in costs among states illustrate the complexity of the issue, they say.
Forty-four states and Washington, D.C., have workers comp medical fee schedules.
While the fee schedules are intended to curb medical costs, George Furlong, chief strategy officer for Sarasota, Florida-based medical bill review company Accuro Solutions, described a balancing act.
“If you have no fee schedule your provider costs are very high,” he said. “If your fee schedule is low, you’re starting to lose providers.”
Most fee schedules pay doctors what they would receive through private insurance or Medicare, Mr. Furlong said, and many states’ fee schedules are based on Medicare (see related story).
Raji Chadarevian, executive director of actuarial research for the Boca Raton, Florida-based National Council on Compensation Insurance, co-authored a report released last month that showed that during the past decade, non-fee schedule states saw doctor fees grow at a faster rate than the national average.
“In general, non-fee schedule states tend to reimburse the same service at a relatively higher amount,” Mr. Chadarevian said.
States without physician services medical fee schedules are Indiana, Iowa, Missouri, New Hampshire, New Jersey and Wisconsin. Some of these states have pharmacy, hospital and ambulatory surgery center fee schedules.
Many states have amended their fee schedules since 2019, according to a June 2022 Workers Compensation Research Institute report. Many update their fee schedules in accordance with laws that require fee schedules to be re-examined, but changes vary.
Maryland, New York, Pennsylvania and Texas had double-digit percentage increases between 2019 and 2022.
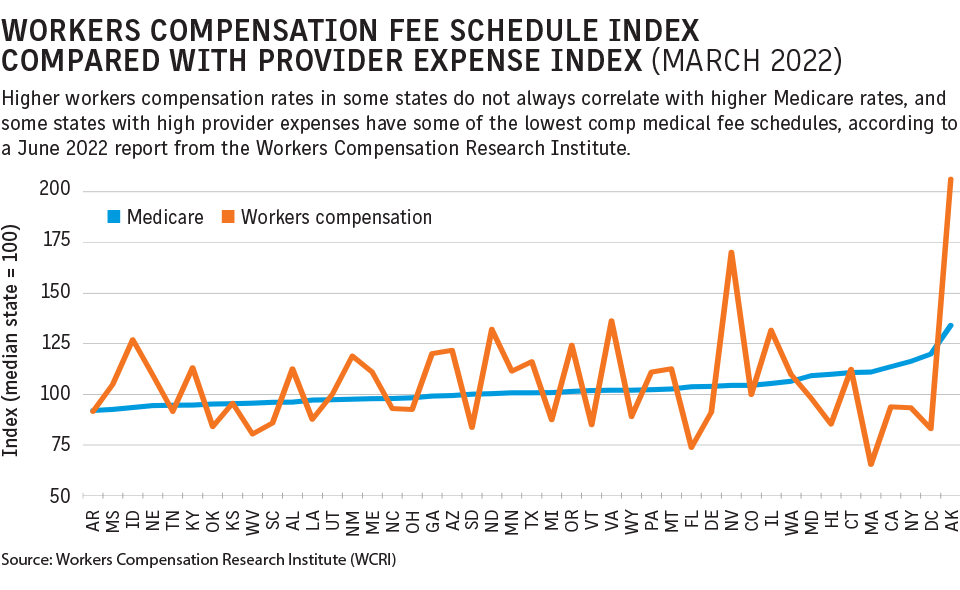
While a majority of states have fee schedules, the percentage paid compared with Medicare varied from 5% below in Massachusetts to 163% above in Nevada, the WCRI report said.
States with some of the highest provider expenses — including California, Hawaii, New York and Massachusetts — had some of the lowest fee schedule reimbursement rates in the country.
Some stakeholders are calling for change.
“I think you’ve got to go back to, what’s the purpose of the fee schedule?” said Kent Spafford, who is a board member of the American Association of Payers, Administrators and Networks and also on the WCRI Disability and Medical Management Program Advisory Board. “Designed properly, a fee schedule should provide enough incentive for a provider to treat an injured worker with a high quality of care.”
Fees for different medical services can affect injured worker outcomes, said Jason Beans, CEO and founder of Chicago-based Rising Medical Solutions, which provides medical cost containment services to comp insurers and employers.
Professional services fee schedules that get “too aggressive” in trying to keep fees low could mean fewer physicians treating comp patients, he said.
“In Illinois, it took forever to get a fee schedule, and, even when we got it, it wasn’t very aggressive,” Mr. Beans said of the fee schedule implemented in 2011.
Illinois lawmakers in January introduced House Bill 1548, which would void existing fee schedules after Aug. 31, 2024, and require the Workers’ Compensation Commission to establish new fee schedules by Sept. 1, 2024.
It’s unclear whether employers in states without schedules pay more in total costs.
In Wisconsin, where there is no fee schedule, “employees have more control over their treating physician, which might contribute to higher medical costs,” said Griffin Murphy, policy analyst with the Washington-based National Academy of Social Insurance. “If employees get better treatment when they have control over their treating physician, however, higher medical costs might be offset by lower indemnity benefits and better return-to-work outcomes.”
An attempt to institute fee schedules has been viewed as interfering with employer rights and causes “significant opposition,” Mr. Murphy said.
Other mechanisms could work, according to Mr. Murphy, who said that with rising medical inflation, insurers charge higher comp premiums. Employers can increase workplace safety measures and lobby state legislators to heighten standards for comp claim approval, he said.
“Both of these may effectively reduce claims and thus serve as protection against increasing medical fees,” he said.
Fee schedules are effective when they recognize market prices and are updated to reflect changes in medical treatment or billing practices, Mr. Chadarevian said.
Mr. Beans said “fee schedules have to be written in a way that they do not create negative incentives, to either limit access to care or to change treatment patterns … or billing patterns,” he said.
Establishing rates varies by state
States with medical fee schedules in workers compensation typically base their rates on Medicare, a reimbursement strategy that reflects problematic past systems and modern-day constraints, experts say.
Many states lack the funds to undertake the research necessary to devise fee schedules that are “meaningful for their particular state,” hence the reliance on basing schedules on Medicare, said Kent Spafford, a board member of the American Association of Payers, Administrators and Networks and the Workers Compensation Research Institute’s Disability and Medical Management Program Advisory Board.
Mr. Spafford said medical inflation, a top comp industry concern, should be cause for updating medical fee schedules.
Medicare, because it is subject to budgets and political maneuvering, does not necessarily change its rates based on medical inflation, he said.
Stacy Jones, senior research analyst with the California Workers’ Compensation Institute, said California hasn’t seen significant medical treatment fee schedule changes recently and that the “basic medical treatment fee schedule is very straightforward.”
Many states’ fee schedules, including California’s, were historically based on the average cost of medical services but this led to problems, she said, which is why many states now base fee schedules on Medicare.
Fee schedules were historically based on “usual and customary” physician charges, but that definition created issues in many states since what providers charged and what they were actually paid for didn’t always equate, Mr. Spafford said.
